EXAMINATION OF
THE
ANTERIOR CRUCIATE LIGAMENT
The function of the anterior cruciate ligament is to prevent the
tibia from sliding forward on the femur.
Three ways of assessing the anterior cruciate ligament are:
-
|
|
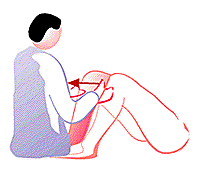
Anterior drawer
test for a ruptured
anterior cruciate ligament.
Have the supine patient flex his
hips to about 45 degrees
so his knees are at about a 90
degrees angle when his
feet are flat on the examining
table.
Sit on the patient's feet and place your hands
around
the upper part of the calf of the limb to be
examined.
Apply an increasingly firm pull on the calf.
|
|
Figure 181
|
|
-
|
|
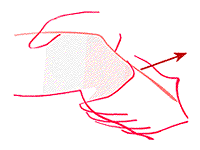
Lachman's test
for a ruptured
anterior cruciate ligament.
Passively flex the knee of the
supine patient to
between 20 degrees and 30 degrees
Hold
the lower part of the patient's thigh in one
hand and the
upper part of the patient's calf in
the other.
Pull the
tibia forward as you would in doing the
anterior drawer
test.
If the patient's thigh is too big to be held by
one
hand, stabilize the thigh by resting it on a pillow,
or
have an assistant hold the thigh with two hands
while you use
your hand or hands to pull on the tibia.
|
|
Figure 182
|
|
-
|
|
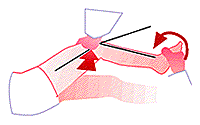
Pivot shift test
for a rupture
anterior cruciate ligament.
Have the patient lying in the
lateral decubitus
position, with the affected knee extended
and
the tibia internally rotated.
Apply a valgus stress to
the knee as you flex it.
A clunk at about 30 degrees of
flexion indicates
a positive test.
|
|
Figure 183
|
|
See (fig
181).
Have the supine patient flex his hips to about 45 degrees so his
knees are at about a 90 degrees angle when his feet are flat on the
examining table.
Sit on the
patient's feet and place your hands around the upper part of the
calf of the limb to be examined.
Instruct the
patient to relax the muscles of his legs (tight hamstrings can mask
a positive sign).
Apply an
increasingly firm pull on the upper calf.
Observe
whether the tibia pulls forward like a drawer opening up. Always
compare with the unaffected side; some normal individuals have up
to half a cm. of play in the ligaments.
If you think the patient has an anterior drawer sign, check the knee
for a sag sign. If the posterior cruciate is torn, you could be
fooled into thinking that the anterior drawer sign was present when
all you were doing was pulling the posteriorly displaced tibia back
into its normal anatomical position.
It is often impossible to hold the thigh and calf as described above
because the patient's thigh is too big for your hand. One way around
this dilemma is to support the thigh on pillows, and then use one or
two hands to move the upper tibia. Alternatively, you can get an
assistant to stabilize the lower thigh with both his hands while you
use your hand or hands to hold and pull on the upper portion of the
lower leg.
Lachman's test is more sensitive than is the anterior drawer sign.
One reason may be that it is difficult for the patient to contract
his hamstrings and thus prevent forward sliding of the tibia when the
knee is in only 20 degrees - 30 degrees of flexion. This is
particularly so if the examiner lifts the whole of the lower leg off
the examining table while performing the test.
The other situation where Lachman's test is used is during the
examination of the acutely injured knee. Often there is a
hemarthrosis and a great deal of pain. One simply can not flex the
knee more than 20 degrees or 30 degrees.
There are undoubtedly many, but I know of only one other that family
physicians should probably know about.
This is the Apley distraction test.
Have the patient lie prone on the examining table with the knees
flexed 90 degrees so the soles of the feet are facing the ceiling.
Holding the
thigh on the examining table, pull firmly upwards on the ankle or
foot thus applying a distraction force to the knee and its
ligaments, and, while doing this, internally and externally rotate
the tibia.
The idea is that such a maneuver should cause pain if the ligaments
are injured. Note that the opposite of the Apley distraction test is
the Apley compression test. The patient assumes the same position,
but the examiner applies a downward compressive and back and forth
rotary force to the knee. The idea is that this grinding pressure
will cause pain if the patient has a torn meniscus.

|
|